

The devil in the details when it comes to interpreting HRV

Repeated release of stress hormones can reduce heart rate variability, the heart’s natural defense mechanism against stress, and literally the beat-to-beat variations of heart rate.
Normally, beat-to-beat intervals change slightly in response to automatic functions such as breathing. The electrical activity of the heart can be measured by waves in an electrocardiogram. The R waves correspond to ventricular depolarization (or electrical discharge of the big chambers of the heart), with the RR interval going from the onset of one R wave to the next one – a complete cardiac cycle. Heart rate variability (HRV) is synonymous with RR variability, and it is regulated by the vagus nerve which is the main nerve of the relaxation response of our nervous system, the parasympathetic system. The sympathetic system with its fight or flight response opposes this relaxing parasympathetic system with the vagus nerve at its main node.
HRV as a marker of vagus nerve activity serves as a measure of inflammation in diseases such as cardiovascular disease. There are several things that can be measured in blood tests to see if a person is inflamed. One of them is C-reactive protein (CRP) which is triggered by the action of inflammatory molecules such as cytokines. The lower your CRP, the higher your HRV. This is why HRV has been strongly correlated with morbidity and mortality in disease. For instance, CRP is a risk factor for myocardial infarction.
It’s not black-and-white
Within this context, high heart rate variability (HRV) means top health and a highly desirable state. However, I did a sleep apnea training a few years ago in one of the best cardiological centers, and I was surprised to learn that in those circles, high heart rate variability at night is a red alert!
The devil is in the details though – one could say that it’s a matter of interpretation and physiological reading parameters. I felt compelled to clarify which was which when I encountered someone whose Oura ring was giving them their highest heart rate variability recorded yet, following what was one of her worst nights due to an asthma attack. We thought at first that the ring was bogus, but perhaps it was just faithfully reporting what it was reading…
First, we need to touch on sleep cycle concepts in order to understand what is going on.
Physio-pathology of the sleep cycle
There are 4 stages during a sleep cycle. In the first stage, there’s still some vigilance, and this is when snoring people can hear themselves. Muscle tone decreases.
During the second stage, muscle tone goes down even further. However, there can be sympathetic activity with blood pressure variations during what are called “K complexes,” which appear during an EEG (electroencephalogram) and come from activity in excitatory cortical neurons. Despite the fluctuations, the important thing to remember is that there’s parasympathetic dominance with decreased sympathetic activity.
In the third stage, there’s very little muscle tonicity. It’s the typical deep sleep when it’s extremely difficult to wake up. There’s dominant parasympathetic activity with reduced sympathetic activity, decreased heart rate, decreased blood pressure, slower respiratory rate, and there’s a moderate drop in cardiac output. Muscle tone decreases even further.
When we transition from stage 1 and 2 towards stage 3, there are parasympathetic outbursts which can translate into certain bradycardias and atrioventricular blockages (when the electrical activity of the heart goes very slow or is blocked altogether).
The last stage is REM (rapid eye movement), which has two activities: the tonic component and the phasic component. The tonic component is always in the background, and it refers to the fact that we are actually “atonic” – that is, we have no muscle tonicity. There’s complete atony of all the striated muscles, except for the diaphragm (we’re still breathing). There’s a very strong cholinergic vagal tonus, with decreased heart rate and blood pressure. Parasympathetic bursts, which can favor sinus pauses (pauses in the heart’s pacemaker) can take place during this stage.
REM’s phasic component refers to cholinergic activity in some centers of the brain stem, which activate the muscles of the eyes and brain centers related to visual imagery (dreams). There are sudden movements of the face and extremities. You can see twitches and micro-awakenings. Here, we can have sympathetic bursts which favor these micro-awakenings. Parasympathetic activity is inhibited. People predisposed to arrhythmias can have ventricular extrasystoles.
During REM, there is increasing sympathetic activity and reduction of parasympathetic activity. Some call it autonomic (“neurovegetative”) storms. There’s variability and there’s cardiorespiratory instability. There’s intermittent low oxygen which can favor increased blood pressure, which can become permanent in people with obstructive sleep disorders such as sleep apnea.
Brain activity variations during sleep have an important role in heart function, specifically on heart rhythm, blood pressure and coronary blood flow. Brutal fluctuations during REM are well tolerated in healthy people, but those with heart disease are at risk of arrhythmias, ischemia and heart attacks. Notice how people with COVID-19 vax-induced-myocarditis died during their sleep…
Deep sleep stages take place more during the first half of sleep, and REM more during the second half of sleep.
Sleep disorders with “high HRV”
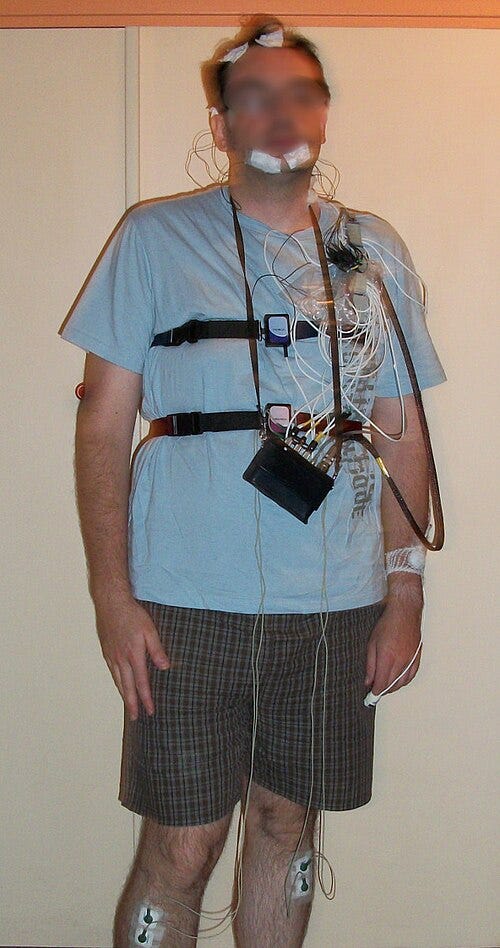
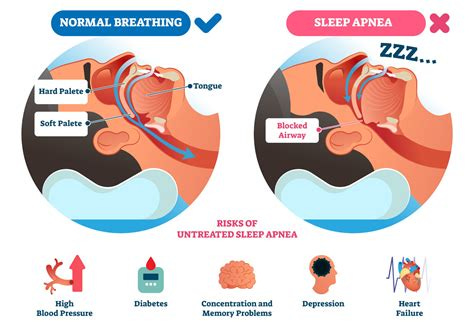
When you monitor sleep disorders, you have at your disposal a nocturnal ventilatory polygraph, which keeps track of your thoracic and abdominal movements, oxygen, heart rate, whether there is air flow in your nose or struggle of air flow in your throat. It also keeps track of your bed position while you sleep. It gives enough information to let you know if there’s struggle while you sleep because there’s too much snoring, because you stop breathing at night or because air flow is just reduced as the tongue collapses your throat due to reduced muscle tonicity, as in this picture:
You can also undergo a polysomnography, which adds many more parameters, including electrical activity in the brain, to know in which exact sleep phase the apnea is taking place.
When reading the heart monitor parameters during sleep and knowing which sleep phase the person is going through, as you do with a polysomnography, if you stumble upon this you can assume the person is in heart health trouble:
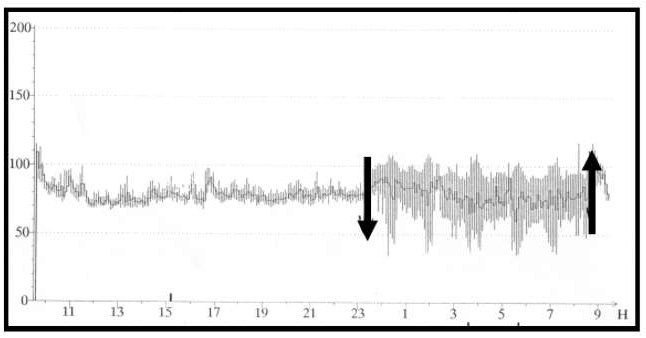
It’s higher heart rate variability of more than 20 beats per minute at night. This person was eventually diagnosed with sleep apnea. And the heart rate variability coincides with stress due to lack of oxygenation during an obstructive flow event. They called it sleep apnea dysautonomia, where the increased heart rate variability alerts the specialist to look for trouble. You go from a parasympathetic predominance with low heart rate while you sleep, to a sympathetic storm due to a micro-awakening while the person struggles to breathe and the heart starts beating much faster. Definition of pathology: higher heart rate variability of more than 20 beats per minute at night.
As the thorax is trying to pump air inside and is fighting against the obstruction at the level of the throat, the heart gets compressed, which stimulates a heart hormone (brain natriuretic peptide). People with these problems get up at night to pee often since the hormone stimulates urination.
You can see sleep apnea in obese people, whenever the ear-throat-nose area is chronically inflamed, and when there are anatomical anomalies such as the amygdalas of the throat or the tongue being bigger than normal. You can also see it in people who had chronic upper airway problems when they were children, which made them chronic mouth breathers. That leads to developmental abnormalities of their facial features, which favors sleep apnea within the context of resistance of the upper airway. There’s actually a syndrome that reveals their sleeping problems, and manifests as follows:
Patients suffering from “resistance of the upper airway syndrome” consult for what appears to be functional problems. They are referred to psychiatrists for management of insomnia, chronic fatigue, muscular disorders labelled as fibromyalgia, headaches, depressive syndromes… all of which represent the most common complaints. Sometimes, in young subjects, unexplained fainting is the revelatory sign of the syndrome [vasovagal syncope]. During this fainting spell, blood pressure tends to be sometimes very low, and the feet, hands and nose are cold. The patients concerned are generally younger than those with the classical obstructive sleep apnea, and complain of bruxism. Their wisdom teeth have often been removed because they were “impacted” between 18 and 25 years of age, and these patients have had orthodontic treatment as teenagers (often inappropriate, as they only consider the dental and not the maxillofacial problems) […]
On examination, they present with a deviated nasal septum, very enlarged lower choanae, and often report respiratory and/or nasal allergic problems. Above all, they have reduced maxillary dimensions, in the upper maxilla, the lower maxilla, or both (with orthodontic problems as a consequence) Guilleminault, Leger : Rev Mal respir 2005 ; 22 : 27-30
It’s similar to a POTS (postural orthostatic tachycardia syndrome), but mechanical in its origin. If problematical enough, surgery is an option. Sometimes physiotherapy is enough.
In summary
Heart rate variability is not necessarily a sign of good health. It depends on which parameters are used for monitoring, and what the context is. Generally, sleep disorder centers are the most advanced at monitoring. Smart rings and other commercial smart monitors have to go to these centers to test their technology and see how they compare to scientific standards. One could argue that heart rate variability as a healthy marker of the smart vagus was never meant to indicate pathology, as monitored above (which is a ‘super-zoomed-in’ version of monitoring). Nevertheless, the lack of consensus among scientists as to what they’re seeing, and the various available interpretations, can give rise to confusion.
In general, commercialized monitors guide and inspire people to be healthier. But those with specific anomalies, as described above, should not be surprised to find high HRV during their ‘worst night ever’. It might be the case that specific medical detective work is needed.
In short, an exception to high HRV as a marker of good health is heart rate variability of more than 20 beats per minute at night, triggered by sleep apnea. The heart rate variability coincides with stress due to lack of oxygenation during an obstructive flow event when the person’s airway shuts down. It’s called sleep apnea dysautonomia and within this context, the increased heart rate variability is a red alert.
A person goes from having a low heart rate within the context of deep parasympathetic relaxation while sleeping, to a high heart rate within the context of a sympathetic storm coinciding with a micro-awakening as the person’s airway shuts down during sleep apnea, triggering an automated struggle to reopen it. This translates as sleep apnea dysautonomia: heart rate goes from very slow to suddenly very fast.
ShareDEC
About the Author:
A countryside family medicine doctor and former heart surgeon in service of the Hippocratic Oath.